Prostate Cancer in Kenya: Rising Incidence, Late Presentation, Screening Debates and Treatment Access at Public and Private Centres
Prostate Cancer in Kenya: Rising Incidence, Late Presentation, Screening Debates and Treatment Access at Public and Private Centres
Prostate cancer has emerged as the most commonly diagnosed cancer among Kenyan men and a leading cause of male cancer death. Recent national cancer estimates place new annual diagnoses in the range of 3,500 to 4,200, with deaths likely between 1,800 and 2,200. The actual burden is probably significantly higher because many cases never reach a hospital that can issue a definitive diagnosis. Most Kenyan men present with advanced or metastatic disease, which sharply limits curative options. This article examines the epidemiology, the biology that explains the African-descent risk pattern, the controversies surrounding population screening with the prostate-specific antigen (PSA) test, the diagnostic and treatment pathway through Kenya public and private health systems, and the role of community awareness, NHIF cover and diaspora support.
Epidemiology and the African-Descent Risk Pattern
Men of African ancestry have higher prostate cancer incidence and worse outcomes globally compared with men of European or Asian ancestry, a pattern observed across the African diaspora and on the continent. The reasons are not fully understood but probably include a combination of genetic variants in the androgen receptor pathway, dietary and lifestyle factors, late access to diagnostic services and differences in tumour biology that produce more aggressive disease. In Kenya, prostate cancer typically presents in men aged 60 and above, although clinically significant cases occur from age 50 onward and a small number of cases present even earlier.
Population data from the Nairobi Cancer Registry and the Eldoret Cancer Registry, both supported by the Kenya National Cancer Institute and academic medical centres, indicate a steady rise in registered prostate cancer cases over the past two decades. Some of the rise reflects population aging and better case ascertainment, but a real increase in incidence is also likely.
Late Presentation and the Reasons Behind It
The most striking feature of prostate cancer in Kenya is that the majority of men present with advanced disease, often with bone metastases or urinary retention at the time of first diagnosis. Several factors contribute. Awareness of prostate cancer symptoms remains low, particularly outside major urban centres. The early symptoms of benign prostatic enlargement, including frequent urination, weak stream and incomplete bladder emptying, can be indistinguishable from early prostate cancer symptoms, and most men assume them to be a normal part of aging. Cultural reluctance to undergo digital rectal examination remains widespread. Access to PSA testing is uneven, with the most reliable laboratories concentrated in Nairobi, Mombasa, Eldoret and Kisumu. Out-of-pocket costs of testing and follow-up are still significant for many households.
PSA Screening: International Controversies and the Kenyan Position
The PSA test measures prostate-specific antigen levels in the blood and remains the principal tool for early detection of prostate cancer. International guidelines disagree on whether population-wide PSA screening reduces overall mortality enough to justify the risk of over-diagnosis and over-treatment, with bodies such as the United States Preventive Services Task Force recommending shared decision-making for men aged 55 to 69. In high-incidence African-descent populations, however, the case for earlier and more aggressive screening is stronger. Kenyan urologists generally recommend a baseline PSA at age 45 to 50 for men with a family history of prostate cancer or African heritage, and at age 50 for the general male population, with subsequent testing intervals based on the initial result. The Ministry of Health has incorporated prostate cancer awareness into the national cancer strategy and has encouraged county health departments to integrate screening into men health outreach.
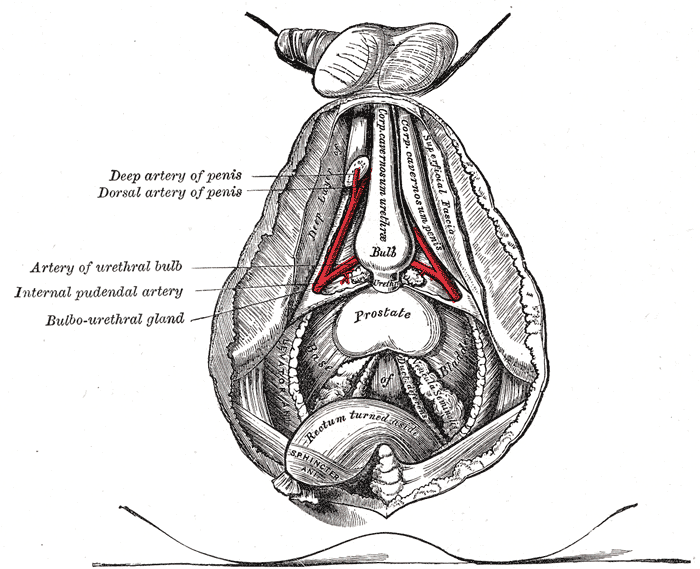
Diagnostic Pathway: From PSA to Biopsy
The standard diagnostic pathway begins with a PSA blood test, often combined with a digital rectal examination. Elevated PSA prompts further work-up, including repeat PSA measurement, urology consultation and transrectal ultrasound-guided biopsy in selected cases. Multiparametric MRI of the prostate is increasingly available in major Nairobi and Mombasa private hospitals, allowing more targeted biopsies and reducing the number of unnecessary procedures. Definitive diagnosis requires histological confirmation by a pathologist, and Gleason grading guides risk stratification and treatment selection.
Kenya has a small but growing community of urological surgeons, medical oncologists, radiation oncologists and pathologists trained to diagnose and stage prostate cancer. The largest concentrations of expertise are at Kenyatta National Hospital, Moi Teaching and Referral Hospital, the Aga Khan University Hospital, the Nairobi Hospital and selected county referral hospitals.
Treatment Options Across the Stages
Treatment depends on stage at diagnosis, patient age and comorbidities, and patient preferences. Localised low-risk disease may be managed with active surveillance, in which PSA and imaging are monitored over time without immediate intervention. Localised intermediate or high-risk disease is typically treated with radical prostatectomy or radiation therapy, increasingly delivered with intensity-modulated or volumetric arc techniques. Locally advanced disease combines radiation with androgen deprivation therapy. Metastatic disease is treated primarily with androgen deprivation, combined with chemotherapy such as docetaxel or with newer hormonal agents such as abiraterone and enzalutamide where available.
Radiation therapy capacity in Kenya is concentrated at the Kenyatta National Hospital, the Moi Teaching and Referral Hospital, the Aga Khan University Hospital, the new Kenyatta University Teaching, Referral and Research Hospital, the HCG CCK Cancer Centre in Nairobi and the Mombasa Cancer Centre. Several county governments are investing in linear accelerators, but capacity remains below international benchmarks. Surgical oncology for prostate cancer, including open and laparoscopic radical prostatectomy, is offered at major referral hospitals.
Cost, Insurance and the NHIF Cancer Package
The financial cost of prostate cancer treatment in Kenya remains a significant barrier for many families. A radical prostatectomy can cost between KSh 250,000 and KSh 1.2 million at private hospitals, depending on technique and facility. Radiation therapy regimens vary from KSh 200,000 to KSh 800,000. Androgen deprivation therapy, once started, continues for months to years and adds to the cumulative cost. The National Hospital Insurance Fund and the successor Social Health Insurance Fund cover inpatient admissions, surgical care, and an oncology benefit package that pays for chemotherapy, radiation therapy and selected hormonal therapies at accredited facilities. Out-of-pocket expenses, particularly for newer agents, remain substantial.
Patient-support organisations including the Kenya Network of Cancer Organisations, the Movember Foundation Kenya programmes and several faith-based hospitals run cost-assistance and patient-navigation services that help newly diagnosed men access timely care.
Awareness Campaigns and Movember
September is Prostate Cancer Awareness Month in Kenya, with the Ministry of Health and partner organisations running awareness campaigns, screening drives and public education events. Movember, the global men health campaign, has supported Kenyan activities since the mid-2010s. Faith leaders, sports figures and corporate champions have increasingly used their platforms to encourage men to seek PSA testing and to overcome the stigma associated with prostate examination. The role of Kenyan mainstream and social media in framing prostate cancer as a serious but treatable disease continues to evolve.
Survivorship, Palliative Care and Quality of Life
Many men diagnosed with localised prostate cancer in Kenya can expect long-term survival following appropriate treatment. Survivorship issues including erectile dysfunction, urinary incontinence, hormonal side-effects, fatigue and emotional well-being benefit from organised follow-up care. For men with metastatic disease, palliative care, including pain management with oral morphine and supportive psychosocial care, is increasingly available through hospice networks coordinated by the Kenya Hospices and Palliative Care Association. Integration of palliative care earlier in the disease trajectory improves quality of life and family coping.
Research and Diaspora Engagement
Kenyan researchers, often working with diaspora collaborators in the United States, the United Kingdom, Canada and South Africa, have contributed to the global literature on the biology of prostate cancer in men of African descent. Studies of the African Caribbean and Black Diaspora population have linked specific genetic variants to higher prostate cancer risk. The Kenyan diaspora has supported PSA testing programmes, contributed equipment to county hospitals, sponsored continuing medical education for urologists and supported patient advocacy groups.
The Way Forward
Reducing prostate cancer mortality in Kenya will require integrated action across awareness, screening, diagnostic capacity, treatment access and supportive care. Sustained public communication that demystifies prostate examination, targeted PSA screening of men over 50 (and earlier with family history or African heritage), more pathology and imaging capacity in county hospitals, predictable supply of androgen deprivation medicines, expanded radiotherapy infrastructure and stronger NHIF cover for the full treatment course are all required. With these investments, the outlook for Kenyan men diagnosed with prostate cancer can improve substantially over the coming decade.
Conclusion
Prostate cancer is the most common cancer in Kenyan men and a growing public health concern as the population ages. Late presentation, screening uncertainty, treatment access limitations and stigma all combine to produce a higher mortality than the disease intrinsic biology demands. Better awareness, targeted PSA screening, decentralised diagnostic capacity and broader NHIF coverage offer a clear improvement pathway. For the diaspora, prostate cancer in Kenya is a tangible cause that combines clinical, philanthropic and family relevance and where modest engagement can have outsized impact.
More Articles

The Multiparty Era Reforms: Saba Saba, the Repeal of Section 2A and Kenya's Return to Political Pluralism
Jul 02, 2026

Eye Care in Kenya: Cataract, Trachoma and the Long Road to Universal Vision Health
Jul 02, 2026

Shaba National Reserve: Joy Adamson's Last Wilderness and Isiolo's Semi-Desert Safari Gem
Jul 02, 2026
The Rendille People of Northern Kenya: Camel Pastoralism, Clan Traditions and a Culture Under Pressure
Jul 02, 2026

Ukulima Sacco: From Ministry of Agriculture Staff Society to a National Cooperative Open to All Kenyans
Jul 02, 2026