Cervical Cancer in Kenya: Burden, HPV Vaccination, Screening Access and the Road to Elimination as a Public Health Problem
Cervical Cancer in Kenya: Burden, HPV Vaccination, Screening Access and the Road to Elimination as a Public Health Problem
Cervical cancer is the second most commonly diagnosed cancer among Kenyan women and the leading cause of cancer death in this group. Each year roughly 5,250 new cases are diagnosed and approximately 3,200 women die of the disease, a mortality rate that ranks among the highest in sub-Saharan Africa. Most cases present at an advanced stage when curative treatment is no longer feasible, reflecting weak primary prevention, low screening coverage and limited downstream treatment capacity. Yet cervical cancer is uniquely vulnerable to public health action. It is caused almost entirely by persistent infection with high-risk human papillomavirus (HPV), it has a long pre-cancer window suitable for screening, and effective vaccines and treatments are available. Kenya has committed to the World Health Organization's global strategy to eliminate cervical cancer as a public health problem by reaching the 90-70-90 targets: 90 per cent of girls fully vaccinated by age 15, 70 per cent of women screened twice in their lifetime with a high-performance test, and 90 per cent of women with pre-cancer or invasive cancer receiving timely treatment. This article examines the current burden, the national HPV vaccination programme, screening modalities, treatment access and the gaps that remain.
Epidemiology and the Disease Burden
The burden of cervical cancer in Kenya is concentrated among women aged 35 to 65, with the modal age of diagnosis in the mid-50s. Co-infection with HIV substantially increases the risk of developing pre-cancer and invasive disease, and the lake counties of Homa Bay, Kisumu and Siaya, where HIV prevalence is highest, carry a correspondingly elevated burden. Nairobi, Mombasa, Nakuru and Kiambu host the largest absolute case loads simply because they have the largest populations. Cervical cancer was responsible for an estimated 17 per cent of all female cancer deaths in Kenya in recent years.
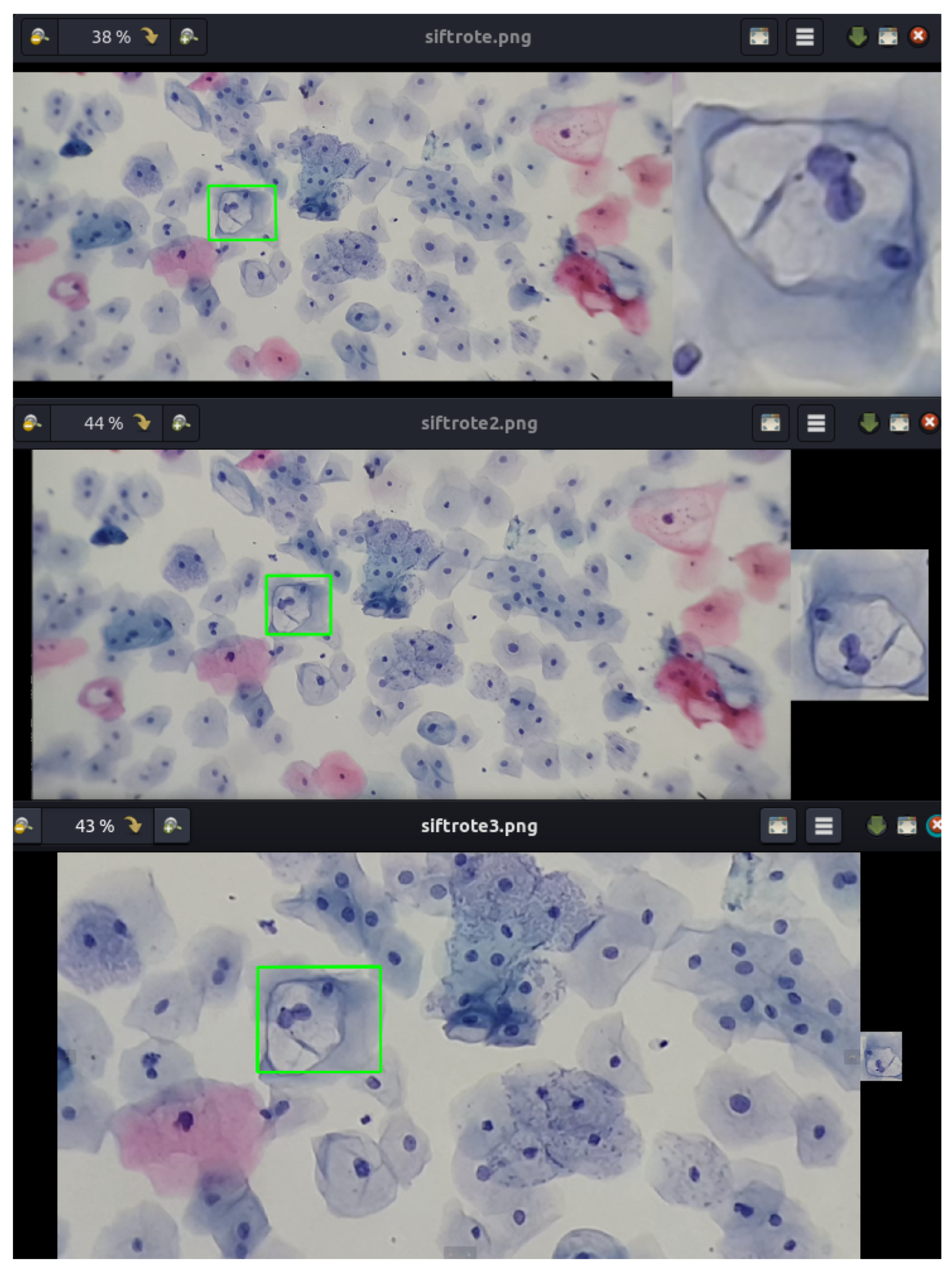
The principal carcinogen is high-risk HPV, with HPV types 16 and 18 accounting for the majority of cervical cancer cases globally and in Kenya. Other oncogenic types including 31, 33, 45, 52 and 58 contribute additional cases. Persistent infection is the necessary cause, but most HPV infections clear spontaneously within two years. A small proportion progress through cervical intraepithelial neoplasia stages over 10 to 20 years to invasive cancer.
The National HPV Vaccination Programme
Kenya introduced HPV vaccination into the routine immunisation schedule in October 2019, targeting girls aged 10. The Ministry of Health partnered with Gavi, the Vaccine Alliance, and Unicef to deliver the bivalent vaccine through schools and community outreach. Initial uptake was constrained by school closures during the COVID-19 pandemic, vaccine misinformation circulated through social media and faith communities, and logistical challenges in reaching out-of-school girls. The Ministry of Health, working with the Kenya Ministry of Health and the National Vaccines and Immunisation Programme, transitioned in 2024 to a single-dose HPV vaccination schedule, simplifying logistics and reducing cost per fully vaccinated girl. Coverage targets remain ambitious: reaching 90 per cent of eligible 10-year-old girls each year requires sustained school-based delivery, catch-up campaigns for out-of-school adolescents, and active counter-misinformation campaigns.
The vaccine is safe, with extensive global post-marketing surveillance demonstrating no causal link to claimed adverse outcomes circulating in misinformation. Parents and faith leaders who have engaged with the evidence have become important champions of vaccine uptake. Civil society and patient advocacy groups, including the Kenya Network of Cancer Organisations and the STOP Cervical Cancer Coalition, support community education.
Screening Modalities and Coverage
Cervical cancer screening in Kenya uses three main modalities. Visual inspection with acetic acid (VIA) or Lugol's iodine (VILI) is the most widely deployed approach, used in over 90 per cent of public facilities offering screening. It is inexpensive, requires minimal equipment and allows immediate treatment with thermal ablation or cryotherapy in the same visit, the so-called single-visit approach. Pap smear cytology is used in some county and faith-based hospitals and many private facilities. HPV DNA testing, the highest-performance modality recommended by the World Health Organization, has been piloted in selected facilities but is not yet routinely available in the public system. Self-sampling kits that allow women to collect a vaginal swab in private and submit it for HPV testing have shown high acceptability in Kenyan studies and may transform screening coverage if rolled out at scale.
Screening coverage remains low. National estimates suggest fewer than 20 per cent of eligible women have ever been screened, far below the 70 per cent target. Reasons include limited awareness, stigma associated with gynaecological examination, fear of pain or embarrassment, opportunistic rather than systematic screening offers, the rural-urban divide in service availability, and out-of-pocket costs even for nominally free public services. Mobile outreach campaigns during Cervical Cancer Awareness Month in October each year reach additional women but cannot substitute for systematic, age-targeted programmes.
Treatment of Pre-Cancer and Invasive Disease
Pre-cancer treatment using thermal ablation, cryotherapy or loop electrosurgical excision procedure (LEEP) is available in major county referral hospitals and several faith-based mission hospitals. The single-visit approach, in which a positive VIA result is treated immediately, dramatically improves loss-to-follow-up rates. Invasive cervical cancer requires more complex care, including radiotherapy, chemotherapy and surgery. Radiotherapy capacity is concentrated at the Kenyatta National Hospital in Nairobi, the Moi Teaching and Referral Hospital in Eldoret, the Aga Khan University Hospital in Nairobi, the Mombasa Cancer Centre and the new Kenyatta University Teaching, Referral and Research Hospital. Several county governments are investing in linear accelerators and brachytherapy suites, but national capacity remains below the WHO benchmark of one teletherapy machine per 250,000 population at risk.
Surgical oncology for cervical cancer, including radical hysterectomy and lymph node dissection, is offered at major referral hospitals and selected private centres. Chemotherapy regimens follow international standard protocols. The cost of full curative-intent treatment for a single patient often runs into hundreds of thousands of Kenyan shillings, much of it currently covered by the National Hospital Insurance Fund and supplementary mechanisms under the Social Health Insurance Fund. Out-of-pocket payments remain substantial for many families.
Palliative Care and the End-of-Life Pathway
For women diagnosed at advanced stages, palliative care is essential. Kenya Hospices and Palliative Care Association coordinates a network of palliative care services across the country, with strong programmes in Nairobi, Nakuru, Eldoret, Kisumu and Mombasa. Oral morphine for cancer pain has become more widely available following advocacy by hospice organisations and the African Palliative Care Association, although stock-outs persist in some counties. Integrating palliative care earlier in the disease course, ideally at the point of advanced diagnosis, improves quality of life and family coping.
Health System and Workforce Considerations
Closing the screening and treatment gap requires investment in the health workforce, including training of nurses to deliver VIA-and-treat, oncologists for tertiary care, pathologists for laboratory diagnosis, radiation therapists and palliative care nurses. Kenya has only a small number of certified gynaecological oncologists, and training pipelines through the University of Nairobi, Moi University and the Aga Khan University need to be scaled. The Cancer Prevention and Treatment Act 2012 and subsequent regulations provide a legal framework, including the establishment of the National Cancer Institute of Kenya.
HIV Co-Infection and Special Populations
Women living with HIV face a fivefold to sixfold increased risk of developing cervical cancer, and pre-cancer progresses more rapidly to invasive disease. The integration of cervical cancer screening into HIV care, through the NASCOP-supported Comprehensive Care Centres, has been a significant success. Most women receiving antiretroviral therapy in Kenyan public facilities can access VIA screening at the same visit. Adolescent girls and young women, sex workers and women in correctional facilities require tailored approaches.
Diaspora Engagement, Philanthropy and Research
The Kenyan diaspora has supported cervical cancer awareness, vaccine procurement, screening equipment and patient navigation services through several Kenya-focused foundations and faith-based initiatives. Diaspora-led research partnerships, particularly between Kenyan academic medical centres and universities in the United States, the United Kingdom and Canada, have contributed to clinical trials, implementation research and capacity building. Continued engagement, including support for HPV self-sampling rollout and rural radiotherapy capacity, can accelerate progress toward the WHO elimination targets.
The Path to Elimination by 2030
The WHO global strategy targets 90 per cent HPV vaccination of girls by age 15, 70 per cent screening of women twice in their lifetime with a high-performance test, and 90 per cent treatment of women with pre-cancer or invasive disease, with measurable progress toward these targets by 2030 and elimination as a public health problem by mid-century. Kenya's current trajectory shows progress on vaccination rollout, growing screening capacity and improving treatment access, but substantial gaps remain. Achieving the targets will require sustained political leadership, increased domestic financing, integration with primary health care, scale-up of HPV self-sampling and rapid expansion of cryotherapy, ablation and LEEP services at sub-county level.
Conclusion
Cervical cancer is a leading killer of Kenyan women, yet it is also one of the most preventable cancers known. With an effective vaccine, a long pre-cancer window suitable for screening, and well-validated treatment protocols, the disease offers a clear public health roadmap. Kenya's commitment to the WHO elimination strategy, the transition to single-dose HPV vaccination, the expansion of VIA-and-treat services, the gradual introduction of HPV testing, and the steady growth of oncology infrastructure mark real progress. Translating this progress into a measurable decline in cervical cancer mortality requires sustained financing, workforce development, community engagement, faith-leader partnership and diaspora support across the next decade.
More Articles

The Multiparty Era Reforms: Saba Saba, the Repeal of Section 2A and Kenya's Return to Political Pluralism
Jul 02, 2026

Eye Care in Kenya: Cataract, Trachoma and the Long Road to Universal Vision Health
Jul 02, 2026

Shaba National Reserve: Joy Adamson's Last Wilderness and Isiolo's Semi-Desert Safari Gem
Jul 02, 2026
The Rendille People of Northern Kenya: Camel Pastoralism, Clan Traditions and a Culture Under Pressure
Jul 02, 2026

Ukulima Sacco: From Ministry of Agriculture Staff Society to a National Cooperative Open to All Kenyans
Jul 02, 2026